Abstract
Background
India continues to face persistent challenges in ensuring affordable and equitable healthcare, particularly in rural areas, where out-of-pocket expenditures remain high. The Indian Government’s Ayushman Bharat–Pradhan Mantri Jan Arogya Yojana (PMJAY) is a flagship initiative toward achieving Universal Health Coverage (UHC), aiming to provide financial protection through cashless secondary and tertiary care. However, awareness, enrolment, and utilisation at the community level are not up to the mark, especially in rural areas. Assessing the level of this awareness, enrolment and utilization and identifying the key barriers are necessary to address this issue.
Objectives:
To assess the levels of awareness, enrolment, and utilisation of the PMJAY scheme among residents of a rural setting in Pune, Maharashtra, and to identify socio-demographic factors influencing these aspects.
Methodology:
A cross-sectional quantitative study was conducted in a rural setting of Pune district, Maharashtra, encompassing eight distinct settlements. A total of 140 respondents aged 18 years and above were selected based on their convenience and availability of respondents at the time of conducting the survey. They were interviewed face-to-face using a structured, pre-tested questionnaire via Google Forms. Data were analysed in Microsoft Excel using descriptive statistics, cross-tabulations, graphical presentation and chi-square tests.
Results:
Of the 140 participants (50% male, 50% female), 70% were aware of PMJAY, while only 42.8% possessed the ABHA card. Awareness was significantly associated with gender and education (p < 0.05). Despite moderate enrolment, no respondent successfully utilised the cashless treatment benefits. Major sources of awareness were government-organised camps (33.67%) and political campaigns (20.41%). Only 13.3% were aware of any empanelled hospitals, and many expressed mistrust due to the rejection of services at the provider level. Barriers to enrolment included perceived lack of benefit, mistrust in the public healthcare system, procedural delays, and dependence on private insurance or out-of-pocket expenses.
Conclusion:
The study reveals that although PMJAY awareness and enrolment have improved, utilisation remains negligible due to systemic inefficiencies and weak health communication. Enhancing digital outreach, improving service delivery, ensuring timely reimbursements, and strengthening community-based engagement are essential to realise the scheme’s potential and advance Universal Health Coverage in rural India.
Keywords:
Ayushman Bharat, PMJAY, Universal Health Coverage, health insurance, awareness, enrolment, utilisation, Out of Pocket Expenditure
Introduction & Background
Providing affordable healthcare while ensuring quality is a major challenge in a diverse country like India. The majority of the Indian population lives in rural India, and most of them have to incur a heavy cost to avail of healthcare services. In addition to this, accessing quality healthcare is not a regular phenomenon, whereas other countries like Cuba and Sri Lanka have achieved significantly better healthcare despite having low GDPs. Ensuring Universal Healthcare Access (UHC) came up as the most feasible and effective option to address the ongoing healthcare issues. [2]
India is one of the worst-performing countries in terms of out-of-pocket medical expenses. The government, in its approach to reducing this burden and ensuring universal access to healthcare, launched the Ayushman Bharat – Pradhan Mantri Jana Arogya Yojana on the 15th of August 2018. The central body which is responsible for running this campaign is the National Health Authority. It is the Nodal Agency which works efficiently in coordination with State health agencies. [2]
The government of Maharashtra started Mahatma Jyotirao Phule Jan Arogya Yojana (MJPJAY) (erstwhile Rajiv Gandhi Jeevandayee Arogya Yojana) on 2nd July 2012 in eight districts on a pilot basis and then it was expanded in all districts of Maharashtra from 21st November 2013. Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) scheme was implemented in integration with Mahatma Jyotirao Phule Jan Arogya Yojana from 2018 to 2020. The government of India and the Government of Maharashtra have been sharing the cost of implementation in the ratio of 60:40. [3]
Meanwhile, the Government of Maharashtra has taken the decision to expand the scope of the current scheme. Accordingly, the integrated scheme is being implemented from 1st July 2024 with an expanded scope as it covers the entire population of Maharashtra. The scheme provides end-to-end cashless quality medical services for identified secondary and tertiary diseases requiring hospitalization through empanelled hospitals. The scheme is implemented on fully Assurance mode. [3]
The key benefits of this scheme are –
- Universal Health Coverage for all citizens of Maharashtra with cashless secondary and tertiary healthcare procedures in govt. and network private hospitals.
- Health coverage of Rs.5 lakhs per year on a family floater basis which means that it can be used by one or all members of the family. All pre-existing diseases are covered from day one.
- Patient can avail treatment in emergency through intimation by telephone or email. [3]
Universal Healthcare Coverage is a guiding light to ensure Sustainable Development Goals across all the world. It helps to improve the overall health of the population of a state and also to reduce impoverishment in healthcare access. The impact and success of any UHC are determined by access to the entire population, ease of enrolment, types of available services, and, finally, ensuring financial protection by reducing catastrophic out-of-pocket spending. [4]
Awareness and Knowledge of both PMJAY and MJPJAY is not up to the mark among the rural population due to less reach of the IEC(Information, Education and Communication) materials. Mass promotion for individual and hospital registration on the portal through Community Health Volunteers and via digital platforms of the Government is required to improve the knowledge, enrolment and proper utilisation of the scheme.[1]
The AB-PMJAY has a huge potential to change the healthcare dynamics in India, particularly by ensuring quality access to poorer and vulnerable populations of society. However, the knowledge and awareness about specific benefits and features of the scheme are comparatively less, which may further lead to less enrolment and underutilisation of the services. [5]
Improper awareness about the PMJAY scheme is an important contributing factor in underutilising the service. The knowledge of the Grievance Cell is very low among the beneficiaries. Knowledge about health government insurance schemes plays a crucial role in influencing the overall coverage and acceptability of the schemes among the beneficiaries. [6]
For a significant portion of Indian households, healthcare services become inaccessible due to high out-of-pocket expenditures. This creates a financial constraint which becomes a restricting factor for seeking medical care. Many families in both rural and urban areas take up bank loans, borrow from friends and families and even sell their assets to overcome health expenditures.
Aim
To assess the level of awareness, enrolment, and utilisation of the Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana (PMJAY) among residents of a rural setting in Maharashtra, in the context of advancing Universal Health Coverage (UHC).
Objectives
The research objectives include:
- To assess the awareness, enrolment and utilisation of the Ayushman Bharat scheme at a rural setting.
- To identify factors affecting the knowledge, enrolment and utilization of the Ayushman Bharat scheme.
Methodology
Study Design:
This study was a cross-sectional quantitative design, which was appropriate for capturing a snapshot of knowledge, enrolment, and utilization patterns of the Ayushman Bharat scheme (Pradhan Mantri Jan Arogya Yojana – PMJAY) among the adult population in the village. The design also allowed for the identification of factors influencing these outcomes by examining associations between socio-demographic variables and awareness or participation levels.
Study Area:
The research was conducted in a village setting, located in one of the Talukas of the Pune district of Maharashtra. It comprised eight distinct settlements along with seasonal migrants living in tents. The settlements were based on either caste/surname or socio economic status.
Target Population:
The target population included all residents of the village aged 18 years and above. Adults were selected as the target group since they are the primary decision-makers regarding health insurance enrolment and utilization in households.
Inclusion and Exclusion Criteria:
The inclusion criteria included –
- Being a resident in the village area for at least one year. For seasonal migrants, it is three months.
- Fall in the age group of more than or equal to 18.
- Agree to participate in the study voluntarily.
The exclusion criteria included –
- Respondents aged less than 18 years.
- Residing in the area for less than one year and less than six months for seasonal migrants.
- Not willing to participate in the study.
Sampling Technique and Sample Size:
One adult respondent was chosen from one household, preferably the head of the household or the person most knowledgeable about the family’s health-related decisions.. The households were chosen based on the convenience and availability of respondents in the house at the time of conducting the survey. A total of 140 responses were taken for the study.
Data Collection Method:
Data was collected through structured, face-to-face interviews. A pre-tested questionnaire was formulated, and the responses were collected by the researcher in Google Forms using a mobile phone. This ensured real-time data capture and minimized data entry errors. The questionnaire was designed to gather:
- Demographic and socio-economic details (age, gender, education, occupation, caste, etc.)
- Knowledge about the Ayushman Bharat scheme (awareness of scheme name, benefits, enrolment process, empanelled hospitals, etc.)
- Enrolment status (whether enrolled, reasons for enrolment/non-enrolment, source of information, experience of enrolment process etc.)
- Utilization of services (if and how the scheme has been used, type of healthcare services availed, satisfaction with the services, barriers faced, etc.)
- Perceived barriers and enablers to improve the knowledge, enrolment, and utilization of the scheme.
Data Analysis:
Data was exported from Google Forms into Microsoft Excel for analysis. The analysis involved:
- Descriptive statistics to summarize the knowledge, enrollment, and utilization levels (e.g., frequencies, percentages, means)
- Cross-tabulations to compare awareness, enrolment, and utilization by socio- demographic characteristics.
- Graphical presentation of key findings using charts and tables to enhance interpretability.
Ethical Considerations:
To satisfy the ethical requirements, the purpose of the study was briefed in understandable language to all the respondents. Only those who had given verbal consent were incorporated into the study. Also, they were assured about the confidentiality of their given data and the anonymity of the respondents was also maintained throughout the study. Although all the respondents were free to opt out at any point in the interview process. No conflict of interest was observed.
Results
Age of the Respondents: The 18-35 group had the highest number of participants with 66 individuals. The 36-59 group had 52 participants. The above 60 years group had the lowest number of participants, with 22 individuals. The average age of the participants was 41.31.
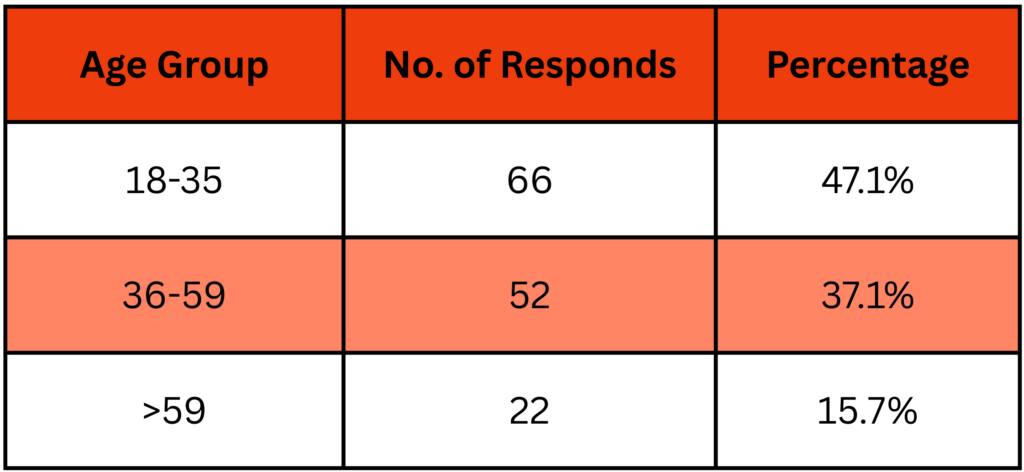
Table 1: Distribution by age
Sex of Participants: The gender distribution was perfectly balanced, with 70 males (50%) and 70 females (50%) respondents, ensuring no gender disparity in the selection process and indicating equal representation of both sexes.
Educational Level: The majority of respondents, 52(37.1%) have completed Secondary education. About 42.2% have pursued education beyond the secondary level, Higher Secondary (26), Graduate (28), or Master’s (5). Rest 29 (20.07%) responded that they have completed till the primary level.

Table 2: Distribution by Educational Qualification
The mean years of schooling for the respondents were found to be 9.3, indicating that the village has a moderate level of education.
Occupation: The largest occupational groups are Farmers (30.7%) and Homemakers (28.6%), together accounting for more than half of the total. Other occupations, such as Business (12.1%), Labourer (10.7%), and Farm Labourer (9.3%), have moderate representation. Salaried employees (3.6%) and self-employed (5%) individuals form the smallest groups.
Table 3: Distribution by Occupation
Caste: The General category forms the majority of participants, 60 (42.9%). About 48.6% the 68 respondents belong to marginalised or reserved categories (SC, ST, OBC), reflecting a significant presence of socially disadvantaged groups. A small proportion (8.6%) of participants were unsure or unaware of their caste status.
Table 4: Distribution by Caste Group
Awareness of PMJAY: Out of the total respondents, 98 individuals (70%) reported being aware of PMJAY. That means they were aware of the scheme name. 42 respondents (30%) indicated they were not aware of the scheme.
Fig 1: Distribution Bar of Awareness
1. Gender Wise Awareness: There is a statistically significant association between Gender and Awareness (χ² = 11.02, df = 1, p = 0.0009). Males are more likely to be aware than females in this sample.
Fig 2: % Distribution Bar of Awareness Gender Wise
Table 5: Chi-Square Table of Awareness vs Gender
2. Education-wise Awareness: Similarly, there is a significant association between education level and awareness of the PMJAY scheme (χ² =19.59, df = 1, p = 0.000009). Individuals with secondary or above education levels are significantly more likely to be aware of the scheme than those with primary or lower education levels.
Fig 2: % Distribution Bar of Awareness Education Wise
Table 6: Chi-Square Table of Awareness vs Education
Source of Awareness: Those who were aware were asked about their source of awareness. Government camps were the primary source of awareness (33.6%), followed by Political Campaigns (20.4%), Community health workers (16.3%), and friends/family (13.2%). Mass media, in the form of TV/Radio (10.20%), Social Media (3.06%), and Newspapers (2.13%), collectively played a minor role, suggesting a need to strengthen public messaging through these channels.
Fig 3: % Distribution Bar of Source of Awareness
Managing Expenses of Unaware Respondents: Among those who were unaware of the scheme’s name, 30 (71.4%) reported relying on their own funds, which constitute out-of-pocket expenditures to cover healthcare expenses. 8 respondents had private insurance (19%), 3 (7.1%) stated borrowing from relatives or friends to meet the expenses, and one said he had sold his property or asset.
Fig 4: % Distribution Bar of Managing Expenses of the Unaware
Awareness of Benefits: Those who were aware, 39.7% identified free hospital treatment, 25.9% of respondents did not know any benefits, and 25.9% perceived health insurance coverage up to ₹5 lakhs as a benefit. 5.7% of the respondents had misconceptions of cash benefits if they fell sick. They have confused it with other government schemes where cash benefits are given if the candidate fulfils certain criteria. 2.8% of the respondents stated that the scheme provides free medicines.
Fig 5: % Distribution Pie of Perceived Benefits of the Scheme
Awareness of Empanelled Hospitals: One of the most important aspects of the scheme awareness is the awareness of the empanelled hospitals. The study reported that A large majority, 86.7%, had no knowledge of any empanelled healthcare providers. Only 13.3% respondents had the idea of nearby facilities.
Table 7: % Distribution by Awareness of Empanelled Providers
Possession of ABHA Card: Beneficiaries are issued a 14-digit Ayushman Bharat Health Account Number along with a PVC card to facilitate smooth availing of services. Those who are aware of the PMJAY scheme, only 60 (61.2%) reported possessing an ABHA card. A significant 38 (38.8%) stated they do not have an ABHA card.
Table 8: % Distribution of ABHA Card Possession
Reasons for Not Enrolling: Among those who did not enrol, a significant number of respondents, 31.6%, didn’t consider the scheme useful to them. Some individuals (21.1%) reported that they are covered by different types of health insurance (private/employer), while others have shown a willingness to enrol soon (15.8%). Around 10.5% stated that they are aware but do not know how to enrol or where to go for enrolment. The rest had miscellaneous reasons, including unawareness of the benefits, missing the enrolment camp, applying but not receiving an ABHA card, and relying on the AFMC Pune.
Fig 6: % Distribution Bar of Non-Enrolment Reasons
Enrolment Process and Experience: The majority of the population, 28 (46.7%), have enrolled themselves through the help of ASHA workers, 18(30%) of them have enrolled through the Enrolment camp in the village, 12(20%) have enrolled through self- registration and the rest, 2 (3.3%) don’t remember how they have enrolled in the past.
Fig 7: % Distribution Pie of Enrolment Process
Most of the respondents, 44 (73.3%), said that the process of enrolment was easy, 14(23.3%) said it was neutral, and the rest,2(3.3%), said that the experience was difficult. Some of the difficulties include a lengthy, time-consuming process and a delayed response after applying (approximately one year).
Fig 8: % Distribution Pie of Enrolment Experience
Scheme Utilisation: Those who possessed an ABHA card, only 6 respondent families (10%) tried to utilise the scheme but faced Card rejection and had to pay from their own pocket. It suggests a lack of a hospital compliance and complaint- raising system. This reflects a poor grievance redressal mechanism at the health system level. 76.7% of the respondents stated that they had not utilised the scheme so far.
Fig 9: % Distribution Bar of Reason for Non Utilisation
Distrust in the quality of care, at 10%, reflects a preference for private healthcare. Two respondents were unable to locate an empanelled hospital, indicating a problem with the dissemination of information.
Discussion
The study in the village setting, which comes under the Pune district of Maharashtra, was conducted with proper representation from all major settlements or wasti (in local dialect). The sample also had a balanced gender ratio(50:50) and diverse age group representation (19-78), which may have enhanced the validity and generalizability of the findings within the village context.
Socio-Demographic Parameters
The educational profile suggests a moderately educated population, with secondary education being the most common and a mean of 9.3 years of schooling. In terms of occupation, farmers and homemakers constituted the largest groups, highlighting the agrarian economy. This occupational pattern also indicates a dependence on agriculture and informal employment sectors, with minimal formal salaried employment. Clearly, this pattern reveals the importance of health insurance support for emergency health crises.
Nearly half of the respondents (48.6%) belonging to reserved categories also highlight the vulnerability and the need for social schemes like PMJAY.
Awareness and Knowledge Gaps about PMJAY
While 70% of participants were aware of the Pradhan Mantri Jan Arogya Yojana (PMJAY), this still leaves a considerable 30% uninformed. The awareness was notably higher among males and those with higher education levels, and both associations were statistically significant. This suggests that health communication strategies may not be equally effective across all social and educational groups. Additionally, awareness of the scheme was mostly limited to the scheme name, with limited knowledge of the actual benefits.
71.4% of the unaware respondents would rely on out-of-pocket expenses to meet their emergency healthcare expenses. This suggests a potential vulnerability to financial stress from medical costs and highlights the need for broader health insurance coverage or financial protection mechanisms.
Information Sources and Communication Gaps
As per the responses, Government-organized enrolment camps (33.6%) and political campaigns (20.4%) were the primary sources of information for the scheme, indicating that formal outreach mechanisms are somewhat effective. However, mass media and digital platforms had minimal influence. There was also a clear communication gap regarding scheme benefits, with only a quarter of respondents (25.9%) correctly identifying the ₹5 lakh coverage. A considerable proportion either misunderstood the benefits or lacked knowledge entirely. This reveals a need for strategic communication outreach campaigns to enhance awareness and enrollment in the scheme.
Knowledge of Healthcare Facilities and Enrolment Issues
There is a glaring lack of awareness about empanelled hospitals and coverage under the scheme. Only 13.3% could name a nearby empanelled hospital. This extremely low awareness is a critical gap in the pathway from scheme awareness to actual utilisation. This will also impact the decision-making during any health emergency at the family level.
Only 60 (42.8%) out of 140 respondents possessed the ABHA card, despite 70% being aware of the scheme, indicating that awareness alone does not translate into enrolment. Significant households without possessing the card show that the Digital health infrastructure and community outreach still need wider penetration.
Several barriers to enrolment were identified, including perceived lack of usefulness (31.6%), preference for private/employer insurance (21.1%), lack of procedural knowledge (10.5%), and administrative or logistic issues (e.g., missed camps or delayed card issuance) (36.8%). These reasons point toward both perceptual and systemic hurdles in increasing the enrolment ratio.
Enrolment Process and User Experience
Most of the enrolments were facilitated by ASHA workers(46.7%) or village enrolment camps(30%), emphasizing the critical role of community health workers and remote enrolment camps. A majority found the process easy (73.3%), but a notable minority complained about issues like delayed processing and inadequate follow-up, which could erode public trust in the system over time.
Utilisation and Systemic Failures
Perhaps the most significant finding of this study is the lack of actual scheme utilisation. Not a single respondent successfully availed of the cashless treatment benefits. Those
who attempted to do so were rejected by empanelled hospitals due to delayed reimbursements. This undermines the fundamental purpose of the scheme.
Further, trust issues were evident, with some respondents expressing doubt about the quality of care under PMJAY and others unable to locate empanelled hospitals when needed. These issues collectively highlight a critical implementation gap, where possession of the ABHA card does not guarantee access or benefit realisation.
Conclusion
The entire study reveals a critical healthcare accessibility gap in the village setting. It shows reasonable awareness and moderate enrolment, but zero utilisation of the scheme. While health communication through different campaigns and community outreach has partially succeeded in creating awareness of the programme, major gaps still remain in awareness of the benefits, empanelled hospital network, enrolment facilitation, and actual service delivery.
To make the scheme more effective at the ground level, multiple approaches are necessary. It may include strengthening communication through digital and mass media, building trust and accountability in empanelled hospitals, ensuring a smooth reimbursement system for empanelled healthcare facilities, and addressing procedural and infrastructural barriers to enrolment and utilisation.
Several interventions are required at the health system level to improve the awareness of the scheme. Only then may it lead to more enrolment and proper utilisation. By critically addressing these systemic challenges, the actual utility of PMJAY as a social health protection mechanism and the ultimate goal of achieving UHC can be fulfilled.
Limitations
Despite showing some interesting facts about the awareness, enrolment and utilisation of the PMJAY scheme, there were some limitations which should be considered. The limitations include:
- The study was primarily focused on the hospitalisation/secondary and tertiary case point of view. So, the primary healthcare aspect is not covered in this study.
- The study was conducted only in the village setting and may have lacked generalisation due to the responses being from the point of view of the villagers only.
- Being time-bound, the number of participants has been less.
- The study was based purely on the knowledge factor as given by the people. Recall bias could be there. The analysis was based purely on the responses given by the respondents.
- Finally, there was a language barrier as the village was located 40km away from Pune city. The villagers were not entirely comfortable with the researcher’s language, which was Hindi/English.
References
1. Manmohan Sharma, Swanand D. Tilekar and Manasi V. Shelgaonkar (2023). To Assess the Knowledge, Awareness and Utilization of People Regarding PMJAY – Ayushman Bharat Yojana and Mahatma Jyotiba Phule Jan Arogya Yojana in Rural Areas of Rahata Taluka, Maharashtra. Biological Forum – An International Journal, 15(5): 62-68.
2. About Pradhan Mantri Jan Arogya Yojana (PM-JAY), National Health Authority, https://nha.gov.in/PM-JAY
3. State Health Assurance Society, Integrated Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana & Mahatma Jyotirao Phule Jan Arogya Yojana, Government of Maharastra, https://www.jeevandayee.gov.in/MJPJAY/FrontServlet?requestType=CommonRH&actionVal=RightFrame&page=undefine d%3E%3E%3Cb%3EMJPJAY%3C/b%3E&pageName=MJPJAY&mainMenu=About&subMenu=MJPJAY
4. Angell BJ, Prinja S, Gupt A, Jha V, Jan S. The Ayushman Bharat Pradhan Mantri Jan Arogya Yojana and the path to universal health coverage in India: Overcoming the challenges of stewardship and governance. PLoS Med. 2019 Mar 7;16(3):e1002759. doi: 10.1371/journal.pmed.1002759. PMID: 30845199; PMCID: PMC6405049.
5. ThomasB,RaykundaliyaDP, BhattS, VadhelK. Study of awareness, enrolment, and utilization of Ayushman Bharat PradhanMantri Jan Arogya Yojana in Gujarat, India. Int J Community Med Public Health2023;10:2741-7.
6. Prof. Umakant Dash, Prof. V R Muraleedharan, Mr. Rajesh M, Accessing Ayushman Bharat- Pradhan Mantri Jan Arogya Yojana (PM-JAY): A case study of three states (Bihar, Haryana and Tamil Nadu), National Health Authority, 2019.
7. Sriee G V VP, Maiya GR. Coverage, utilization, and impact of Ayushman Bharat scheme among the rural field practice area of Saveetha Medical College and Hospital, Chennai. J Family Med Prim Care. 2021 Mar;10(3):1171-1176. doi: 10.4103/jfmpc.jfmpc_1789_20. Epub 2021 Apr 8. PMID: 34041146; PMCID: PMC8140258.
8. Ghosh, S. (2020). Implementation challenges of Ayushman Bharat: Evidence from early experiences in Indian states. Indian Journal of Public Health, 64(3), 223–227.
https://doi.org/10.4103/ijph.IJPH_453_19
9. Basu, S., Andrews, J., Kishore, S., Panjabi, R., & Stuckler, D. (2012). Comparative performance of private and public healthcare systems in low- and middle-income countries: a systematic review. PLOS Medicine, 9(6), e1001244. https://doi.org/10.1371/journal.pmed.1001244
10. National Health Authority (2022). PM-JAY Annual Report 2021-22. Government of India. https://nha.gov.in/pmjay-reports
11. Bajpai, V., & Wadhwa, M. (2021). Health insurance in India: A study of awareness, coverage, and utilization of Ayushman Bharat in Uttar Pradesh. Journal of Health Management, 23(4), 607–622. https://doi.org/10.1177/09720634211056156
12. Prasad S, Singh C, Naik B N, et al. (March 08, 2023) Awareness of the Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana in the Rural Community: A Cross-Sectional Study in Eastern India. Cureus 15(3): e35901. doi:10.7759/cureus.35901
13. Parisi, D., Srivastava, S., Parmar, D., Strupat, C., Brenner, S., Walsh, C., Neogi, R., Basu, S., Ziegler, S., Jain, N., & De Allegri, M. (2023). Awareness of India’s national health insurance scheme (PM-JAY): A cross-sectional study across six states. Health Policy and Planning, 38(3), 289-300. https://doi.org/10.1093/heapol/czac106
14. Srivastava, S., Bertone, M.P., Basu, S. et al. Implementation of PM-JAY in India: a qualitative study exploring the role of competency, organizational and leadership drivers shaping early roll-out of publicly funded health insurance in three Indian states. Health Res Policy Sys 21, 65 (2023). https://doi.org/10.1186/s12961-023-01012-7
15. V., A., K., U. G., M., P., Maiti, R., M., A., & C., M. P. (2021). Oral health utilization and awareness of Ayushman Bharat (PMJAY) health insurance scheme in Bangalore. International Journal Of Community Medicine And Public Health, 8(8), 4012–4018. https://doi.org/10.18203/2394-6040.ijcmph20213037
16. Saikia, B., Pal, M., Ringkangmai, W., & Krishnan, S. (2023). A quasi-experimental study to assess the effectiveness of planned teaching program on knowledge regarding Ayushman Bharat Yojana among community people in Panchayatan village, Greater Noida, Uttar Pradesh. International Journal Of Community Medicine And Public Health, 11(1), 157–164. https://doi.org/10.18203/2394-6040.ijcmph20234119
17. Reddy, N. K. K., Bahurupi, Y., Kishore, S., Singh, M., Aggarwal, P., & Jain, B. (2020). Awareness and readiness of health care workers in implementing Pradhan Mantri Jan Arogya
Yojana in a tertiary care hospital at Rishikesh. Nepal Journal of Epidemiology, 10(2), 865–870. https://doi.org/10.3126/nje.v10i2.27941
18. Sankar G K, Mahendran R. Expanding AB-PMJAY For the Elderly: A Policy Shift Toward Universal Health Coverage in India. Natl J Community Med [Internet]. 2025 Jun. 1 [cited 2025 Oct. 27];16(06):646-9. Available from: https://njcmindia.com/index.php/file/article/view/5287
19. Garg, K., & Sharma, M. (2023). Exploring the Degree of Awareness of Medical Insurance and AB-PMJAY within Blue Collar Workers in Gurugram . Journal of Student Research, 12(1). https://doi.org/10.47611/jsrhs.v12i1.3991
20. Jeetendra Yadav, Savita Devi, Mahesh Nath Singh, Navneet Manchanda, Moradhawaj, Health care utilization and expenditure inequities in India: Benefit incidence analysis,Clinical Epidemiology and Global Health,Volume 15,2022,101053,ISSN 2213-3984
21. Kalita A, Carton-Rossen N, Joseph L, Chhetri D, Patel V. The Barriers to Universal Health Coverage in India and the Strategies to Address Them: A Key Informant Study. Annals of Global Health. 2023; 89(1): 69, 1–17. DOI: https://doi. org/10.5334/aogh.4120
22. Mehak Nanda, Rajesh Sharma, A comprehensive examination of the economic impact of out-of-pocket health expenditures in India, Health Policy and Planning, Volume 38, Issue 8, October 2023, Pages 926–
938, https://doi.org/10.1093/heapol/czad050
How to Cite This Article
Karmakar S. A quantitative study on awareness, enrolment and utilisation of Ayushman Bharat PMJAY scheme in a rural setting under Pune district, Maharashtra. PharmaShots. 2026 [cited 2026 Jan 30]; DOI: 10.5281/zenodo.19045754, Citation ID: PS-RP-2026-001: https://pharmashots.com/31171/a-quantitative-study-on-awareness-enrolment-and-utilisation-of-ayushman-bharat-pmjay-scheme-in-a-rural-setting-under-pune-district-maharashtra/